- Controversial issues that affect the dental implant dentistry
Analysis Of The Shortcomings Of The
Hiossen® Implant System
- Gerald Niznick
I had a phone exchange with a Dentist using Hiossen implants. He was defensive when I listed some of the limitations of that system. Here, in greater detail, is what I conveyed to him:
1. Strength of the Titanium: Hiossen’s 3.2mmD implant is made from Ti6Al4V medical grade titanium alloy whereas its 3.5mmD implant, and all its wider implants, are made from Grade 4 titanium which is 36% weaker. There is only 0.01inch difference in wall thickness between the 3.2mmD and 3.5mmD implants which is the thickness of 2 human hairs. The wall all thickness for both small diameter implants is virtually the same because the diameter of the hex on the 3.2mmD implant is smaller than the hex on the 3.5mmD implant. There is no justification for using the alloy with the 3.2mmD but not the 3.5mmD.
3.5mmD Implant with 2.5mmD hex = 1.0 mm/2 = 0.5mm wall thickness 3.2mmD Implant with 2.1mmD hex = 1.1mm/2 = 0.55mm wall thickness

2. Hiossen’s implant System includes three body designs differing primarily in the degree of taper. Their implants from 3.5mmD to 7mmD all have the same internal connection diameter. To create a more hygienic and esthetic emergence profile, the 6mm and 7mm implants have a back-taper at the top. This will leave a gap at the crest of the ridge at the time of placement that could encourage down-growth of soft tissue and sacrifice stability from reduced contact with crestal cortical bone.

3. The threads and blasted surface of all the Hiossen implants extend to the top of the implant. Bone recession and remodeling will result in the threads and blasted surface being exposed to the soft tissue. This can also occur from insertion in an uneven ridge. Exposing the rough surface to the soft tissue as well as the exposed threads has been documented to contribute to peri-implantitis. Hiossen apparently recognizes this as a potential problem as indicated by its surgical protocol which recommends sub-crestal placement of the implant. This not only sacrifices cortical bone support, it also positions the implant-abutment junction subcrestal where micro-leakage can further contribute to bone loss.

4. Hiossen implants have a “Single Pitch Thread” which takes twice as long to screw in as double-lead threads commonly found on most US made implant systems.
5. Only the “Ultra Wide” implants are available in 6mm lengths because of the depth of the internal connection.
6. Hiossen does not have a US Customer Service and Support Center. All calls are routed to a salesperson in the field. It also does not have online ordering or even an online catalog with prices. I made contact with a few of their salespeople and learned that the price of Hiossen implants, made in the U.S, is $330 compared to $250 if the implant is made in Korea. The salesperson informed me that, for the implants made in the U.S., I would get a 47% discount to $174 with a $10,000 pre-paid order. That price dropped to $135 with a $50,000 prepaid order. If I wanted to buy their implant made in Korea, the price with a $50,000 pre-payment was only $83. The U.S implant claims to have a hydrophilic surface created by some process that the two salespeople could not explain. On line I see that they claim it is more hydrophilic by applying a 10u application of HA which resorbs with time. Many implants claim to have a hydrophilic surface but research does not document any clinical advantage. Many implants with porous or rough blasted surfaces exhibit blood running up the surface on insertion. This is called capillary action and can be enhanced by pre-wetting the surface with an alkaline solution.

Here is the Doctor’s response to my critique of the Hiossen Implant System:
1. “Hiossen makes a 6mm long implant so you are factually incorrect.”
RESPONSE: Only for its “Ultra Wide” 6mm and 7mm diameter implants.
2. “I have no issues with Grade 4 pure and do not place into the situation that would overstretch the limitations of the implant.”
RESPONSE: Hiossen makes its 3.2mmD implant from Ti Alloy but its 3.5mmD implant from Grade 4 titanium, which is 36% weaker. Both implants would be equally susceptible to fracture given their wall thicknesses differ by only 0.02 inches. It is only logical that anyone would want to use the strongest implant material at all times rather than guess which applications will not “overstretch the limitations of the implant”.
3. Polished collar is not new and IMO is sub-optimal for today’s concepts.
RESPONSE: I assume “IMO” means “In My Opinion”. In dentistry, an opinion is only as good as the science on which it is based and the credentials of the person expressing that opinion. You are a GP out of dental school for 6 years. In all deference, my opinion is based on 50 years of implant experience, a MSD degree in Prosthetics and Dental Materials, and 33 U.S. Dental Implant-related patents. My implant design which you refer to as “sub-optimal for today’s concepts” has a machined, anodized collar (not polished).
4. Sand blasting the top works well when placed subcrestal which is exactly why I would not place your proposed design.
RESPONSE: Because Hiossen’s threads and blasted surface extend to the top, in order for it to “work well” you need to follow Hiossen’s surgical protocol and place the implant subcrestal. That is the tail wagging the dog. Because of Hiossen’s faulty design that could contribute to peri-implantitis, you further compound the problem by placing the implant subcrestal. What will you do if the ridge is uneven… place it sub-crestal on the lingual or on the labial? Here is a link to a linkedin post where I responded to this very situation. Furthermore, if an implant is placed subcrestal, a counter-sink is often needed to widen the crestal bone in order to attach a flared healing collar and abutment. That unnecessarily adds another step to the surgical procedures and unnecessarily removes bone. Furthermore, if leakage at the implant abutment junction occurs from flexing of the weak, pure titanium implants, screw loosening, or just poor precision, that leakage will be occurring sub-crestal rather than in the gingival sulcus.
5. It is purely conjecture to assume there would be quality control issues from Korea.
RESPONSE: I talked to a Hiossen sales person and learned that a dentist could buy their implants made in the U.S. for $330 or the ones made in Korea for $250 ($80 less). Since the implants are virtually identical, I am even more concerned as to which implant I would be getting if I ordered from that company. My concern about quality control of discount implants from some foreign countries is based on my 40 year involvement in manufacturing and selling implants around the world. I know what it takes to consistently manufacture a high quality implant and those resources and regulatory controls are not readily available everywhere. My factory in Calabasas California was the home for products now sold by ZimVie and Implant Direct/NobelBiocare.
Paragon ordered 30 CNC machines, with an additional $46,000 computer monitoring system added to each machine to assure precision. No other company in the dental implant industry is using this technology. It facilitates lights-out 24/7 production, making a perfect part every time. This efficiency is what will allow Paragon to bring a high quality, innovative implant to the market at only $100. Below is a brochure on the use of Lasers to treat peri-implantitis. The rapid expansion of implant placement by GPs, and the growing number of implant failures, is what brought me back to the industry.


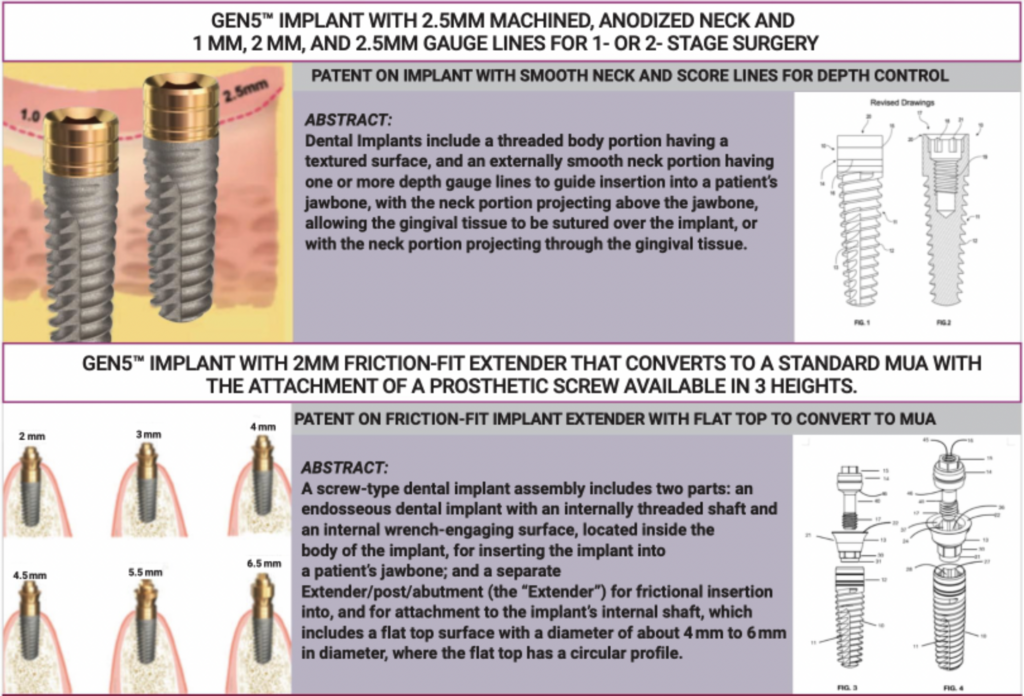
EVOLUTION AND INNOVATION: THREE PATENTED FEATURES OF THE GEN5™ AND GEN5+™ IMPLANTS

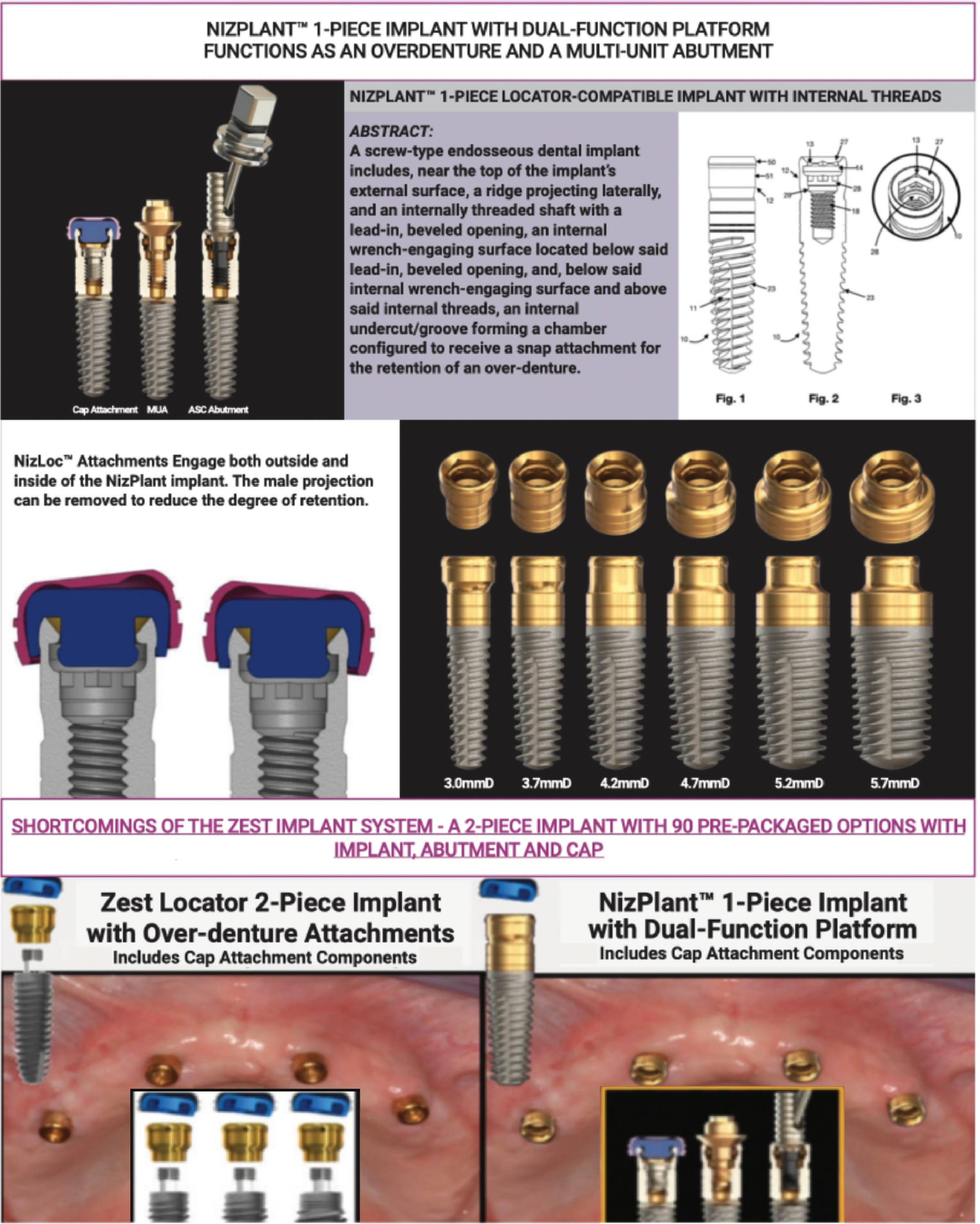
PATENTED FEATURES OF THE 1-PIECE NIZPLANT™ IMPLANT WITH ITS DUAL-FUNCTION PLATFORM

Related Posts
Our mission is to provide high-quality, innovative, dental implants and abutments through internet sales at factory-direct prices.
GET TO KNOW US
LET US HELP YOU
STAY CONNECTED
- Contact Us
- info@paragon-implant.com
- 855.NIZ.GEN5
- Mon-Fri 6am-5pm PST