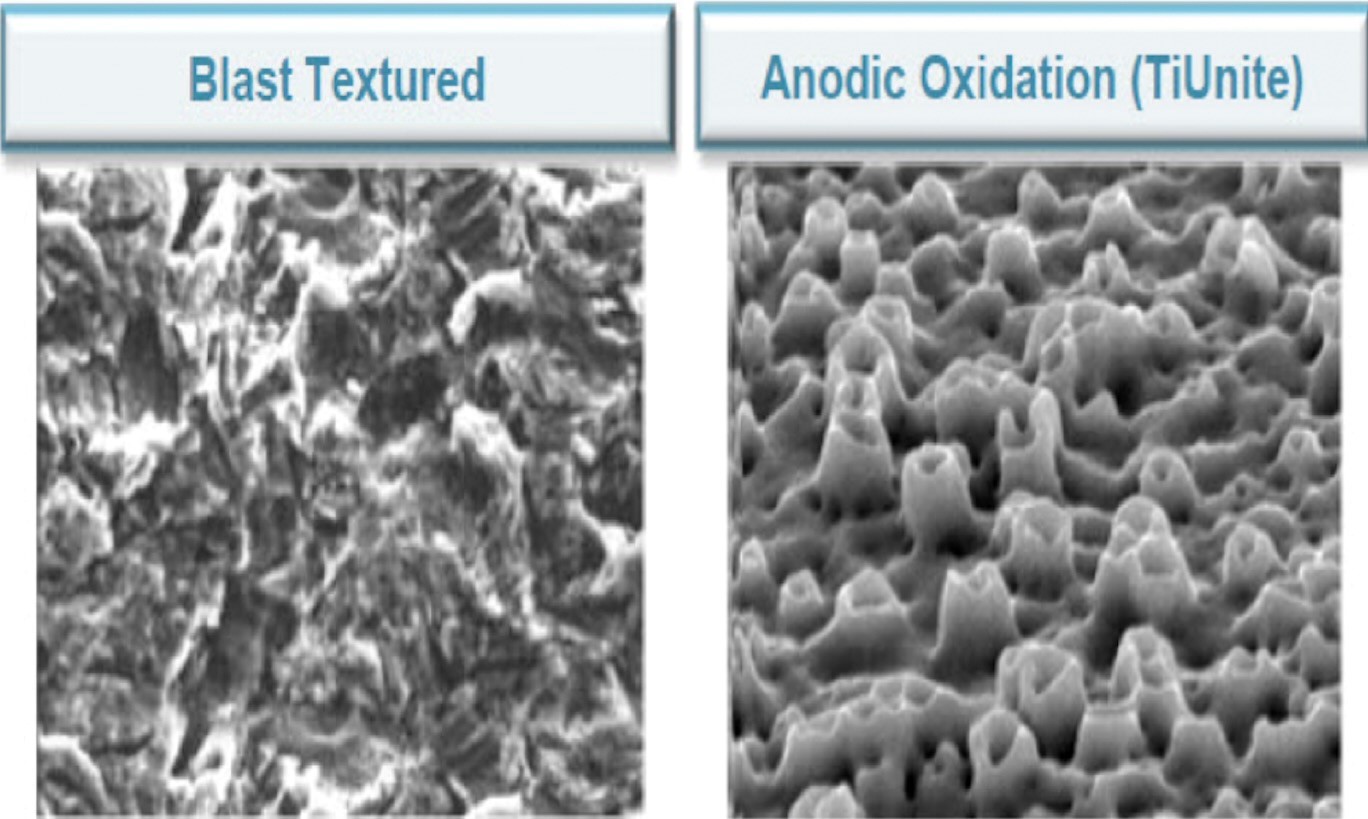
The NobelActive™ implant was introduced in 2008. It has an internal hex connection with a 78° lead-in bevel. It could not be launched in United States until after October 2007, when the internal Conical Connection Patent, Niznick 1990, expired. The Implant was introduced with an anodized, porous surface to the top of the implant, which NobelBiocare® called TiUnite™. In 2020, because of numerous clinical reports of bone loss and soft tissue complications(peri-implantitis) associated with the exposure of the porous TiUnite. NobelBiocare offered the NobelActive, as well as the rest of its implant designs, with a machined, anodized 2mm collar, which they called TiUltra™ surface. This was accompanied with a price increase and as of September 2024, there is a $19 price differential between the original and hybrid surface designs. Having a smooth neck on the implant, called a hybrid design, is well supported by research. Nobel also anodized the surface of its abutments, called it Xeal™, and claimed it enhanced soft tissue attachment, which they called Muco-integration™. These claims are highly questionable as anodizing titanium just changes the refective nature of the surface, not its texture.

The NobelActive System primarily consists of 3 implant diameters, 3.5mmD, 4.3mmD and 5.0mmD. The 3.5mmD implant has a 3.0mmD platform while the other two have a 3.4mmD platform. NobelBiocare also offers a 3.0mmD implant with FDA restrictions for use only for replacement of laterals and incisors, and a 5.5mmD implant, available in a few shorter sizes with the TiUltra surface. This wider implant is primarily for the posterior. These two additional sizes are of limited value considering that the difference in diameter between the 3.0mmD > 3.5mmD, and the 5.0mmD > 5.5mmD is only 1/2mm in cross-section and 1/4mm on each side. 1/4mm = 0.010” or 10 thousandths of an inch, which is about the thickness of 2 human hairs. Soft bone in the anterior could easily be expanded by that amount when inserting a 3.5mmD implant and that minimal difference will not be significant in placing an implant into a posterior extraction socket or in providing additional support for a restoration in the molar area.

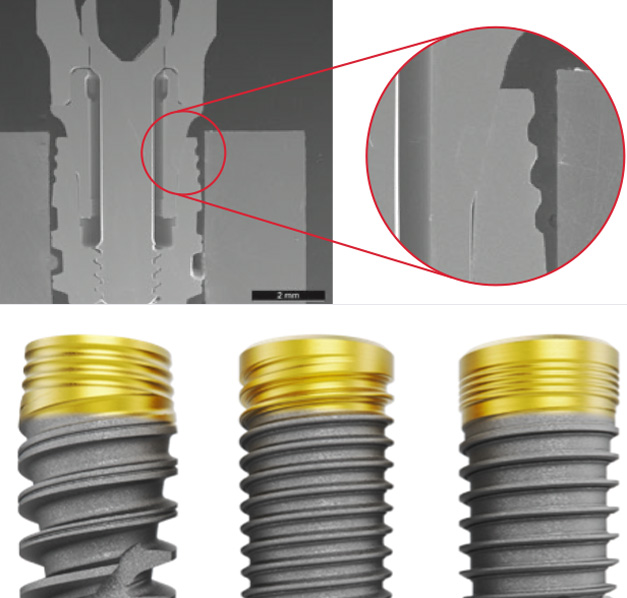
The internal conical connection of the NobelActive has a 78° lead-in bevel as measured from the horizontal, which is 12° as measured from the vertical. This is a variation of the original 45° Conical Connection introduced with the Screw-Vent Implant in 1986. Increasing the angle of the lead-in bevel does not increase stability because, to assure a seal at the opening to the internal shaft, the mating bevel of the abutment is .5° less, as measured from the vertical. In other words, the primary contact between the abutment and the implant, regardless of whether the lead-in bevel is 45° or 78°, is only at the opening of the internal shaft. The steeper bevel has two negative consequences: (1) it thins the walls of the implant, and (2) it deepens the hex within the internal shaft by at least 1mm, limiting the development of very short (6mm) implants. The shortest implant offered by NobelBiocare with the NobelActive implants, other than the widest 5.5mmD implant is 8.5mm.